 Italiano
Italiano English
English
AN INNOVATIVE GENETIC TEST TO PREDICT TESE OUTCOME IN NON-OBSTRUCTIVE AZOOSPERMIA

Identifies the genetic causes of NOA and estimates the probability of sperm retrieval.
Azoospermia and NOA
Azoospermia - defined as the absence of spermatozoa in the ejaculate - is the most severe form of male infertility and affects approximately 1% of the male population.
Etiological classification
Obstructive azoospermia (OA)
sperm production is preserved, but an obstruction of the seminal tract prevents sperm from reaching the ejaculate.
Non-obstructive azoospermia (NOA)
a primarily testicular disorder, with quantitative/qualitative impairment of spermatogenesis up to complete absence of spermatozoa in the ejaculate.
NOA: why this matters for the specialist
In clinical practice, NOA is among the most challenging conditions in male infertility management: in many patients the only option to obtain gametes suitable for ART (ICSI) is surgical testicular sperm retrieval via TESE / micro-TESE, which nevertheless fails in a substantial proportion of cases (≈50% in idiopathic series).
Clinical-hormonal parameters and first-line genetic tests (karyotype, AZF microdeletions) provide limited prognostic value, except for selected conditions (e.g., complete AZFa or AZFb/bc deletions).
In recent years, Next Generation Sequencing (NGS) has enabled the identification of monogenic determinants of NOA and, crucially, the correlation of specific genes with the likelihood of sperm retrieval.
WHAT IS FERTILADVANCE TESE
FERTILADVANCE TESE is an advanced genetic test designed to identify the genetic causes of NOA and to estimate the probability of sperm retrieval, providing prognostic stratification of TESE/micro-TESE outcome.
Main purposes

Identification of monogenic causes associated with NOA/spermatogenic failure through the analysis of 200+ genes involved in key spermatogenic pathways (meiosis, recombination, chromosomal synapsis, germ cell maturation, flagellar structure, etc.).

In the presence of pathogenic variants in specific genes with evidence supporting TESE−/TESE+ association:
TESE-negative (very unfavorable prognosis):
genes consistently associated with failed retrieval in carriers of pathogenic variants → may support avoiding repeated invasive procedures with an unfavorable risk/benefit ratio.
TESE-positive:
genes compatible with residual sperm production and possible (variable) retrieval → TESE/micro-TESE may be clinically justified, with outcome influenced by the specific gene, phenotype, and/or histology.
Genes associated with TESE-negative outcomes and clinical implications
By integrating multicentre cohorts and the scientific literature, genes have been identified in which pathogenic variants are recurrently associated with failed sperm retrieval (TESE-negative).
Main genes associated with TESE-negative outcomes in carriers of pathogenic variants
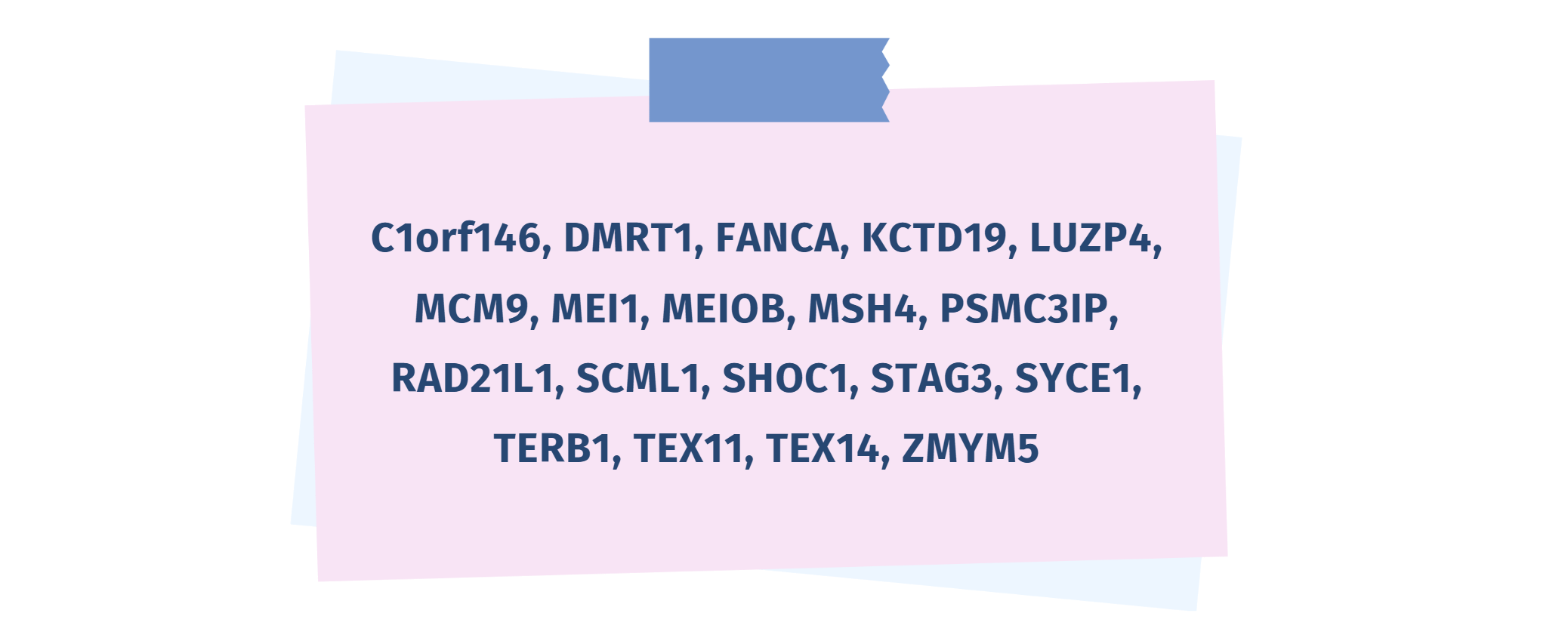
Many of these genes encode proteins essential for meiosis and recombination (chromosomal synapsis, crossing-over, DNA repair), or for the early germ cells progression. Defects in these pathways may result in severe maturation arrest and absence of mature germ cells available for retrieval.

Clinical implications
A pathogenic variant in these genes is indicative of a very low likelihood of sperm retrieval by TESE—close to zero for some genes (e.g., TEX11, SYCE1, and MSH4).
In these cases, clinical counseling may include:

discussion of whether to avoid repeated invasive procedures with low expected benefit;

consideration of alternative strategies (e.g., male donor sperm), according to patient preferences and the clinical-legal context.
Riera-Escamilla et al. Genetic determinants of testicular sperm extraction outcomes: insights from a large multicentre study of men with non-obstructive azoospermia. Hum Reprod Open. 2025 Aug 29;2025(3):hoaf049.
Genes associated with TESE-positive outcomes and clinical implications
Genes have also been identified in which pathogenic variants are compatible with residual sperm production and therefore with a possibility of retrieval (TESE-positive).
Main genes associated with TESE-positive outcomes in carriers of pathogenic variants

Clinical implications
A pathogenic variant in these genes does not rule out sperm retrieval and suggests partially preserved or intermittent spermatogenesis: TESE/micro-TESE may be clinically justified, with variable success.
Retrieval probability may be gene-dependent and influenced by clinical/histological factors: for some genes, success has been reported in up to approximately half of cases, whereas for others the probability remains low but not null.
Riera-Escamilla et al. Genetic determinants of testicular sperm extraction outcomes: insights from a large multicentre study of men with non-obstructive azoospermia. Hum Reprod Open. 2025 Aug 29;2025(3):hoaf049.
Test results
Positive: pathogenic variant detected
Supports the molecular diagnosis of NOA/spermatogenic failure.
If detected in TESE−/TESE+ genes, contributes to prognostic assessment and clinical decision-making.
Negative: no pathogenic variant detected
Does not exclude a genetic basis for NOA, given its high genetic heterogeneity and the possibility of variants in regions not interrogated.
Clinical decisions should be based on the overall andrological evaluation.
Indications for testing
NOA after comprehensive andrological work-up and exclusion of obstructive causes.
NOA with non-informative first-line testing (karyotype, AZF).
Pre-TESE evaluation for prognostic counseling and clinical decision-making.
Previous TESE-negative result for etiologic reassessment and re-definition of reproductive strategy.
Severe oligozoospermia/cryptozoospermia when considering surgical retrieval and/or fertility preservation.
Need for reproductive genetic counseling (TESE/ICSI, cryopreservation, alternatives).

Turnaround time:

brochure

Request information about FERTILADVANCE TESE test
Fill out this form for a free consultation. One of our geneticists will contact you, free of charge and with no obligation, to provide you with all the information you need.
